Genu valgum in children.
Genu valgum is one of the reasons why an orthopaedic assessment is most frequently required in children. “My son has X-shaped knees, is that normal? Can we do something?”
In most cases these are physiological conditions for which it is enough to reassure parents. Yet, in some cases, more attention is required.
PHYSIOLOGICAL DEVELOPMENT OF THE KNEE IN CHILDREN
Typically the lower limbs of newborns show a slight varus axis, which is more evident when the infant starts to stand, with consequent concern of the parents.
The axis then tends to improve spontaneously, reaching the neutral axis around 18-24 months and then continuing towards valgus deviation, with a peak around 3.5 – 4 years.
Finally, valgus deviation decreases again and gradually returns to the mild physiological valgus of the adult’s knee.
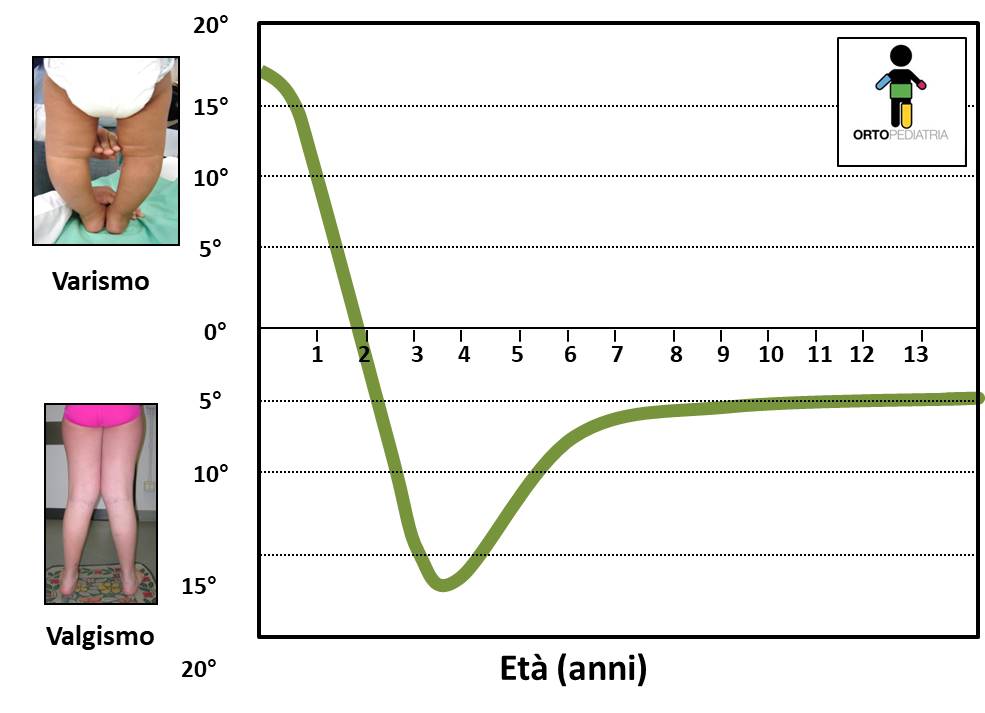
This description obviously corresponds to an average of healthy subjects, so it is possible to find small variations from the average. For example, it is common to find children with slight deviation (with respect to the graph), without this falling into a pathological picture.
The genu valgum: evaluation.
The simplest and most immediate way to evaluate the genu valgum is to make the child stand with his thighs touching (that is, the two thighs must not be forced to tighten) and the feet separated. Patellae should look forward. Knees should not be flexed.
In this way you will immediately visually have the idea of the condition. We advise parents to take photos periodically (every 6 months) in this position from front and back to keep track of the situation over time without performing radiographs.
In this position one can evaluate the angle between the thigh and the leg (difficult to measure) or alternatively measure the Inter-Malleolar Distance (IMD), that is the distance that separates the two malleoli.
This is an empirical measure affected by many parameters (correct positioning of the child or the presence of fat thighs, etc), but has the advantage of simplicity and can allow to monitor the progression of axis over time.
In general, an IMD below 6-8 cm is considered physiological, always considering all the aspects (age, trend, overweight, etc).

Idiopathic and secondary genu valgum
IDIOPATHIC
Some children, after the completion of the physiological development of the knee axis (then after about 8 years), continue to present, even in the absence of underlying pathologies, an excessive valgus knee.
This can lead to problems, in particular: obstacles in walking and running, patellar disturbances, stress on the ligaments on the medial side of the knee and aesthetic disturbances.
If not corrected, over time can lead to excessive overload with wearing of the cartilage of the knee.
SECONDARY
Genu valgum is due to an underlying pathology. Some examples are:
• Rickets. It is among the most frequent forms
• Mild hypoplasia of femur (congenital short femur)
• Post-traumatic valgus: following a fracture
• Skeletal dysplasia: metaphyseal, spondyloepiphyseal, etc
• Multiple exostosis: see relative page

Treatment of genu valgum in children
For most children with genu valgum it is enough to reassure parents and consider good standards of personal care and active life (attention to overweight, sports practice, use of appropriate footwear, etc.).
Do the orthopaedic shoes and orthotics work? Effectiveness has never been proven.
Are the night braces working? No, and they are poorly tolerated by children.
Surgical interventions: epiphysiodesis and osteotomies.
For more pronounced cases of valgus knee, corrective intervention should be considered.
In preparation for surgery, radiographs are performed to calculate the mechanical axes.

Asymmetrical epiphysiodesis
It’s a simple and very effective procedure if done properly. Metallic tools (the most frequent is the “eight-plate”) are applied on the medial (=internal) side of the growth cartilage of the knee in order to slow the growth in this area. The remaining cartilage in the lateral part continues to grow and leads progressively to the correction.
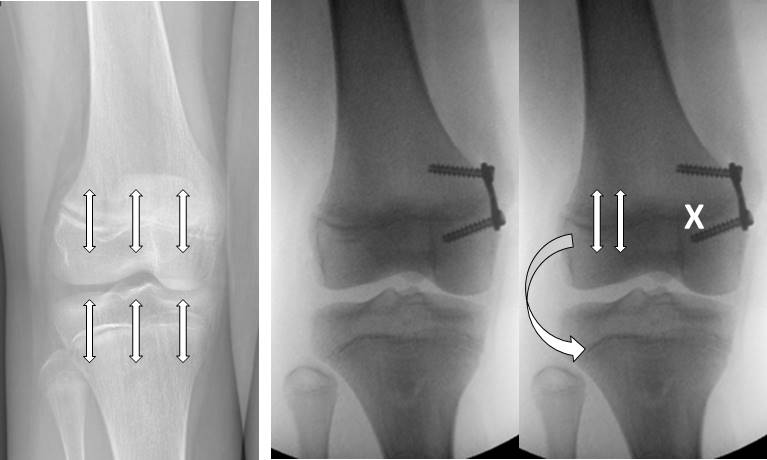
The plates can be placed at the femur (more frequently) and/or tibia based on the site of deformity. The correction of the axis does not occur directly in the operating room, but progressively with time: the speed is proportional to the growth of the operated limb.

The basic requirement is that the child has residual growth.
It’s a minimally invasive procedure, it doesn’t need immobilization or plaster, you can do it on both knees at the same time. Patients quickly recover walking and return to sporting activity within a few weeks.
It is a temporary procedure: once the desired objective has been reached (that is, once the axis has been corrected), plates are removed and the physis is supposed to start to grow again.
However, two possible risks must be considered.
- The risk of lesions of the growth cartilage produced by the plate itself: once the plates are removed, the knee will still deviate in the direction of correction, leading to hyper-correction
- The rebound effect: Once the plates are removed, cartilage starts to grow too much, leading to a recurrence of the deformity.
For this reason, it is necessary to perform the procedures with the correct technique, timing and indications.
Corrective osteotomy for genu valgum
It is a very effective surgery for the treatment of valgus knee, but more challenging than the epiphysiodesis. Bones are corrected and fixed in the new position by metallic tools (Kirschner wires, plates, screws, etc.).

Take a look at:
Back to Pediatric Orthopedics