A particular case of genu varum: Blount disease.
Blount disease is a growth disorder of the medial (=internal) side of the growth cartilage of the proximal (=upper) tibia in children, which causes a progressive genu varum.
Due to this disorder the medial part of the growth cartilage slows down its activity, while the outer part continues to grow. This leads to a gradual varus deformity with severe deformation of the knee.
Two forms are distinguished, based on the age of appearance:
- the most frequent form affects children with onset before 8-9 years (usually around 2-3 years). Typically the child shows a rapid progression of varus deformity during the second/third/fourth year of life.
- more uncommonly, adolescents are affected (onset after 9-10 years).
Blount disease may affect one side (unilateral) or both sides (bilateral)

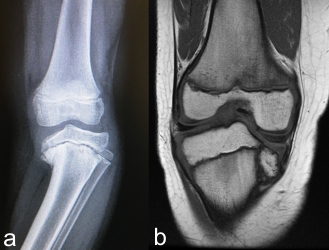
The axis of the limb shows a sharp varus deviation immediately under the knee. The leg has an internal torsion, so that the foot shows an internal rotation with respect to the knee
Blount disease should be differentiated from the physiological varus knee and from other forms of secondary varus knee. For this purpose, radiographic examinations may be performed.
Once the diagnosis of Blount disease is established, treatment should be undertaken promptly.
Treatment of Blount disease
In mild cases of Blount disease at an early stage (usually up to 3 years), a conservative treatment (brace) may be attempted and can be effective in some cases.
In case of failure, in severe cases and in older children, surgical treatment must be quickly performed, to avoid progression of the pathology.
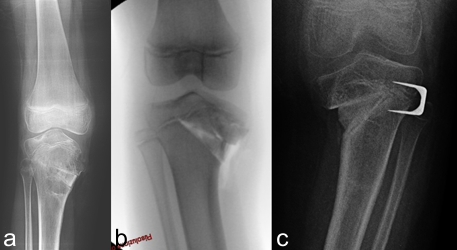
Surgical procedures are tailored to the pathological findings in the single patient. Typical features are: deformation of the articular surface of the tibia (the internal part is lowered with respect to the external one), the varus deviation, the deformation of the distal femur, the shortening of the limb, etc.
Surgical treatment of Blount disease is complex and requires experience to limit errors and incomplete corrections.
Given the growth disturbance in the medial part of the physis of proximal tibia, the deformity has the tendency to recur with growth
The main procedures that can be performed are:
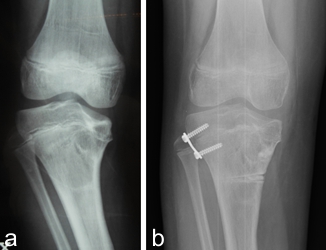
• Valgus osteotomy of the proximal tibia: indicated especially in cases operated early. It is associated with risks of neurovascular disturbances.
• Elevation of the medial tibial plateau: indicated when the joint surface is deformed, to restore the profile.
• Double tibial osteotomy: includes the two previous procedures, to simultaneously treat both the varus deviation and the joint deformity.
- Lateral asymmetrical epiphysiodesis with “8” plates. A plate is placed in the lateral part of the growth cartilage of the tibia.

- Progressive correction with external fixator. This is a complex technique with excellent results, especially for the most severe cases. It allows the simultaneous correction of different aspects (varus, internal rotation, shortening) and limits neurovascular complications
Take a look at:
Back to Pediatric Orthopedics