What is the Perthes Disease?
Perthes disease (or Legg-Calvè-Perthes disease) is a condition where an ischemic event affects the vascularization of the femoral head (epiphysis) during growth, causing an “avascular necrosis”. In simpler terms, blood does not reach the femoral head adequately and bone cells die.
As a result of this event, Perthes disease leads to a rather typical scenario in which initially the femoral head slows down its development and tends to crush and fragment, and then restructures and remodels progressively in a more or less satisfactory way.

CAUSES OF PERTHES DISEASE
The causes of Perthes disease are not known, although several factors have been called into question (coagulation alterations, vascular microtraumas, primary abnormalities of the ossification of the epiphysis, etc.).
The process affects males much more frequently (male to female ratio = 4:1) and generally only on one side (about 85% of cases). It is not a hereditary disease: familiarity is positive very rarely (5%).
Perthes disease can occur in a very wide age group (between 2 and 13 years) but typically affects children between 4 and 8 years.
CLINIC FEATURES
Initially the child shows limping and generally complains of pain in the groin or thigh or knee.
Very important: in a child who complains of knee pain, you should always consider that the pain can come from the hip.
Pain has mechanical features, that is, it resolves with rest and increases with activity.
There is no fever, no general discomfort. Blood tests are normal.
On examination: the affected hip has a restricted range of motion (reduction of abduction and rotations above all).
HOW TO DIAGNOSE PERTHES DISEASE?
The differential diagnosis of includes other diseases that most frequently affect the hip of children in the same age group, mainly transient hip synovitis and osteoarticular infections. After the initial examination, blood tests, ultrasound and finally an x-ray will guide the physician towards the correct diagnosis.
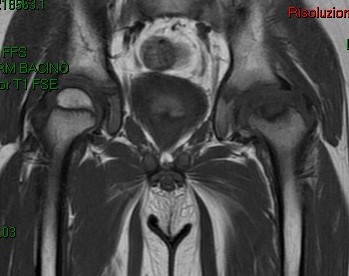
At an early stage of Perthes disease, however, it is possible that radiographs still does not show signs of Perthes disease.
In these cases a Magnetic Resonance Imaging is more sensitive in showing the early process.
THE TYPICAL EVOLUTION THIS DISEASE
Perthes disease has a typical radiographic evolution: the femur goes through several phases:
1. Early phase: increased density of the femoral head epiphysis
2. Fragmentation phase: the nucleus appears fragmented, due to resorption of necrotic trabeculae
3. Reparative phase: re-ossification begins
4. Healed. The proximal femur gradually reaches its final form.
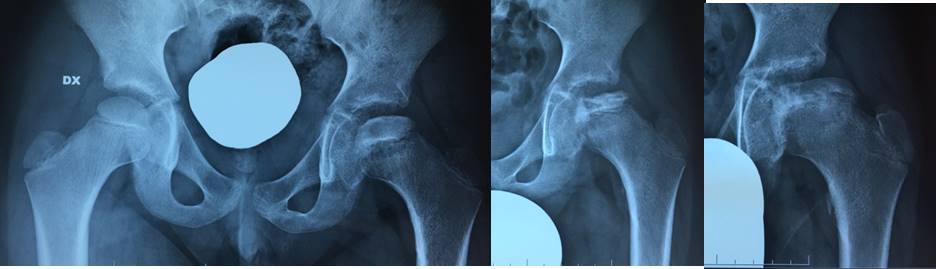
final shape of the femoral head is as spherical and congruent as possible with respect to the acetabulum.
In the event of an outcome in not-spherical, ovoid or not congruent forms or macroscopic alterations of the femoral neck (coxa magna, coxa plana, coxa brevis) this will result in more serious alterations of the joint and subsequent premature degenerative arthritis.
“RISK FACTORS” FOR PROGNOSIS IN PERTHES DISEASE
The prognosis is mainly linked to:
• Clinical signs of hip at risk: obesity, contracture in adduction, etc
• Radiographic signs of hip at risk: Gage sign, metaphysitis, tendency to subluxation, lateral calcifications, etc
• Severity of the involvement. This is evaluated according to the classification of Herring (or lateral pillar classification) which subdivides into groups with increasing gravity (A, B, B/C borderline, C) and prognosis progressively worse, depending on the involvement of the lateral part of the epiphysis.
It is important to note that the severity, according to the Herring classification, can only be assigned from fragmentation phase. This means that in cases with early diagnosis of Perthes disease, this classification cannot be used to guide treatment and evolution.
The conservative treatment: the objectives. What is “containment”?
Main objectives of treatment are:
• Short-term: maintain joint movement as much as possible.
• Mid-term: Keep the femoral head centred in the acetabulum.
• Long-term: retain the sphericity of the femoral head at the end of growth.
The “containment” is the basic principle of the treatment of patients with Perthes disease: by keeping the head of the femur in the acetabulum (with brace or surgery), the acetabulum works as a mold to keep the head of the femur spherical.
The femoral head in Perthes disease has in fact the tendency to subluxate (that is, to move laterally outside the acetabulum in a progressive way) and in the most serious cases develops a deformity of its lateral part (Hinge Abduction) which prevents the head from re-entering completely inside the acetabulum.
CONSERVATIVE TREATMENT
It includes several tools:
• Physiotherapy
• Periods of traction (night, full-time) to reduce muscle contraction
• Swimming pool, exercise bike
• Load limitation: use of crutches/wheelchair to limit deformation/collapse of the femoral head
ARE BRACES USEFUL IN PERTHES DISEASE?
In the past, different types of braces have been proposed (Thomas brace, Atlanta brace, TDA, etc.). However, none of these braces have shown to be effective.
Moreover, they are also very challenging for families and patients. To date they have been almost completely abandoned.
Surgical treatment for Perthes Disease
To keep the femoral head centered in the acetabulum, the orthopaedic surgeon should evaluate the best surgical procedure (osteotomy of the femur or pelvis). Each procedure includes advantages and disadvantages, which the orthopaedic surgeon will need to know well and discuss with the family.


IS IT THE OSTEOTOMY ALWAYS NECESSARY?
No. The orthopaedic surgeon will need to consider the various aspects of Perthes disease (age, severity, risk factors, stage, etc.) to decide the type of treatment.
For most cases no treatment is recommended and conservative treatment is sufficient.

In some cases, release of the retracted muscles or a dynamic arthrography will be considered to better assess whether the head of the femur has the possibility of centration or not.
WOULD IT BE BETTER TO WAIT AS LONG AS POSSIBLE FOR THE SURGERY?
Unfortunately, that’s a misconception. Surgical intervention for Perthes disease should be considered before or during the initial stages of fragmentation, therefore rather early. One of the most frequent errors is to decide too late to operate, when the head of the femur has deformed, with very poor results.

Back to Pediatric Orthopedics